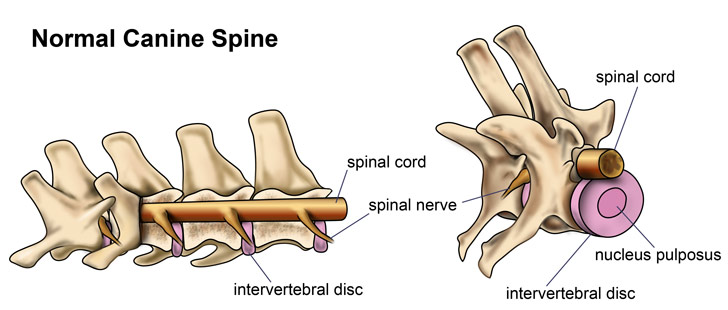
IIVDD stands for intervertebral disc disease. It is also known as herniated disc(s) or ruptured disc(s). A dog’s backbone is made up of individual bones, or vertebrae, that form a tube, within which the spinal cord is protected. Discs are the joints that connect the vertebrae to one another. They are soft in the center and have a tougher outer layer. The spine helps bear the weight of the animal and also needs to move in many different ways. The job of the discs is to work as shock absorbers for the vertebrae.
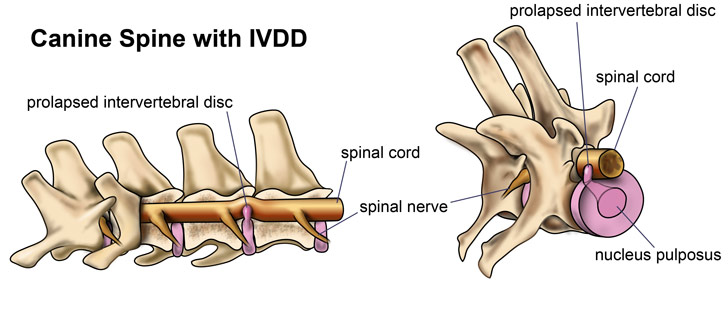
In IVDD, the material on the inside of the disc, the nucleus pulposus, degenerates over time. There are 3 main types:
- Type I: The disc material oozes upwards from the more fibrous outer case, the annulus fibrosis, toward the spinal cord. This material can then push either on the nerve roots that exit the spinal column and connect to the rest of the body or on the spinal cord itself. This causes pain, nerve damage, and paralysis to the area that is enervated by the affected part of the spine. This can occur anywhere along the vertebral column, from the neck to the lower back. Surgery generally carries a good prognosis for this type of disc disease.
- Type II: This is a slower process where the outer fibrous layer weakens but does not tear. Then over time (often months to years) the disc bulges into the canal. This typically occurs in older, larger breed dogs. Surgery is less often recommended.
- Type III: In this scenario a very small amount of disc material ruptures very rapidly and impacts the spinal cord at a high rate of speed. This results more in a ‘bruising’ type injury rather than compression of the spinal cord. Surgery is usually not necessary.



There are two elements affecting the spinal cord’s response (i.e. severity of symptoms) to a disc extrusion. One is the velocity with which the disc hits the spinal cord when it ruptures. Disc material can ooze out of the disc space into the canal like toothpaste and cause very little impact injury to the spinal cord or it can explode out of the disc space into the spinal canal striking the spinal cord with a high velocity or high forceful impact, creating severe spinal cord damage or even permanent paralysis. Continued cellular cord injury processes are ongoing for up to 5-7 days following the impact injury sustained the moment the disc ruptures and hits the spinal cord regardless of surgical intervention. Less then 1% chance of death or permanent paralysis is estimated due to on going impact/velocity injury to the cord (myelomalacia) from the disc extrusion despite surgical intervention or complications from possible spinal diagnostics and surgery. The second injury process is directly related to the volume of disc material emptied into the canal squeezing the spinal cord. If a small volume of disc material ruptures into the canal with low force or low velocity, the spinal cord can accommodate and surgical intervention is not indicated. If a high volume or large amount of disc material ruptures into the canal under any force, the spinal cord will be continually injured if this disc material is not removed from the canal as soon as possible. Emergent surgical intervention is aimed at removing the disc material from the canal to make the canal environment as optimal as possible so if the cord can recover from the impact/velocity injury, it can without being continually squeezed by disc material. Removing ruptured disc material from the canal sooner rather than later decreases the chances of continued injury effects as the spinal cord is continually squeezed by a moderate to large amount of disc material extruded into the canal. A delay in the removal of disc material from the canal can result in permanent decreased functional reserves within the spinal cord and can decrease recovery to the fullest potential if surgery is pursued at a later time.
A grading scale is used in dogs to document the severity:
- Grade 0) Normal
- Grade 1) Pain only–these dogs are able to walk normally, but exhibit signs of pain including reluctance to move, reluctance to jump, shivering, crying, muscle spasms, and/or a tense abdomen.
- Grade 2) Ambulatory paraparesis–these dogs are able to walk, but are weak and wobbly in the rear legs. They may cross their back legs when walking, splay out, knuckle over or stumble in their back legs.
- Grade 3) Non-ambulatory paraparesis–these dogs are still able to move their legs and wag their tails, but are not strong enough to support their own weight and walk.
- Grade 4) Paraplegia–these dogs have no voluntary movement in the rear legs.
- Grade 5) Paraplegia with absent nociception (no ‘deep pain’)–in addition to being unable to move the back legs, they are unable to feel their back legs.

There are other diseases that can cause similar clinical signs of spinal cord disease including meningitis/myelitis, spinal tumors, trauma, infection, malformations, and vascular problems. A thorough neurological examination can give the veterinarian an idea of hich of these are more likely than others, but tests are necessary to accurately determine the cause. Spinal radiographs are useful for screening for disk infection and bony tumors, but typically are insufficient to diagnose intervertebral disk disease. Magnetic resonance imaging (MRI) is considered the imaging modality of choice when visualizing the nervous system.
Treatment for IVDD generally involves either a medical / conservative approach or a surgical approach. Conservative care can be used for IVDD if the dog is still able to walk and has appropriate pain reflexes. In this case, anti-inflammatory and pain medications and strict rest may help to resolve the IVDD. Strict rest involves confining the dog to a cage or small area where she can’t get up or move around. The owner must be diligent with nursing care in this case, bringing food and water to the dog, and carrying her out and supporting her for urination and defecation. Strict rest is usually required for about 4-6 weeks. After that time is taken to gradually increase the dog’s activity level back to near normal. However, any activity that involves jumping should be removed from the dog’s life for good because the risk is just too high of another disc herniation.
Surgery is almost always necessary for dogs that are not able to walk anymore or do not have appropriate pain responses. These things indicate that the connection between the brain and the nerves to the affected limb are no longer working, and surgery is necessary to relieve the pressure on the affected nerve.
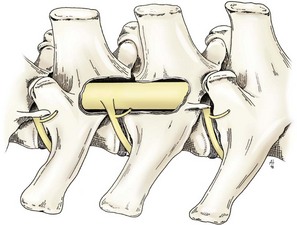
Hemilaminectomy
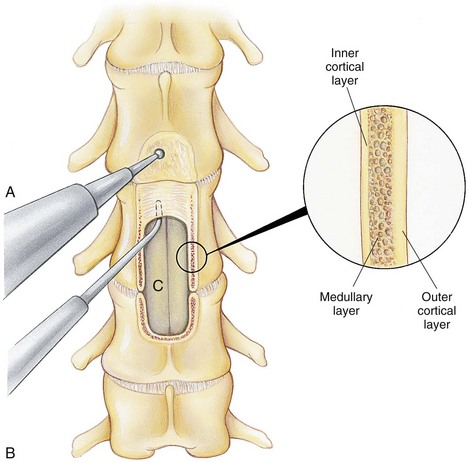
Ventral slot
Physical therapy is helpful during conservative treatment and after surgical treatment. It must be done with care to ensure that your dog does not suffer further injury. There are veterinary physical therapists in many areas, including facilities that can do underwater therapy, which has very good results. Where they are not available, your veterinarian can teach you some specific physical therapy exercises and tell you how often to perform them at each stage of recovery.Acupuncture has been used as part of the physical therapy for dogs during conservative care or after surgical treatment for IVDD. Many people feel that it helps speed healing.
The prognosis for IVDD in dogs varies depending on the severity of the signs and how quickly treatment is initiated. Dogs that can still walk and retain their pain reflexes have a good chance (~60-75%) of recovering with conservative treatment. However, they also have a much higher chance of the problem recurring than if they are treated surgically. Dogs that present as Grade 1-4 generally have a good prognosis with surgery (90-90%). Dogs that don’t feel pain in their feet are a surgical emergency. Even with surgery, these dogs have a lower chance of recovering than dogs that don’t lose deep pain reflexes.

