Discospondylitis is a bacterial or fungal infection of the discs between the vertebrae (intervertebral discs). This infection can occur in any area of the spinal column, and it can occur at multiple sites. Discospondylitis is also known as spondylitis, intervertebral disc infection, and vertebral osteomyelitis. Discospondylitis occurs much more often in dogs than in cats.
The bacterial/fungal infection can reach the intervertebral disks several ways:
-
Through the bloodstream, which is the most common method. (Chronic infections of the skin, urinary tract, prostate, etc. can result in bacteria entering the bloodstream and traveling to the disk area.)
-
Via direct contamination from punctures or bite wounds near the spine, or from procedures or surgery near the spine.
-
From the migration of foreign bodies through the area near the spine.
Often the exact source is never found.
Signs
Neurological signs have a gradual onset and are progressive. At the beginning, spinal pain, stiffness, unsteady walking, and other nervous system problems may occur. Spinal pain is the most consistent clinical sign. Impaired movement (paresis) is usually mild, unless the infection gets into the spinal canal. However, if the pet doesn’t get appropriate treatment, signs can progress to paralysis, often caused by fractures of the vertebrae. The muscles alongside the spine may atrophy (waste away); this is most likely due to local nerve damage or associated myositis (muscle inflammation).
Spinal cord compression can be caused by granulation tissue, bony changes, or fractures or dislocations (luxations) due to the infection. The vertebral fractures or dislocations may require surgery to stabilize them.
Occasionally, the infection may result in meningitis, meningomyelitis, or an abscess in the spinal canal.
Diagnosis
Diagnosis may require radiography, advanced imaging modalities (CT scan, MRI, bone scintigraphy), urinalysis, bacterial cultures, serology, and cerebrospinal fluid analysis.
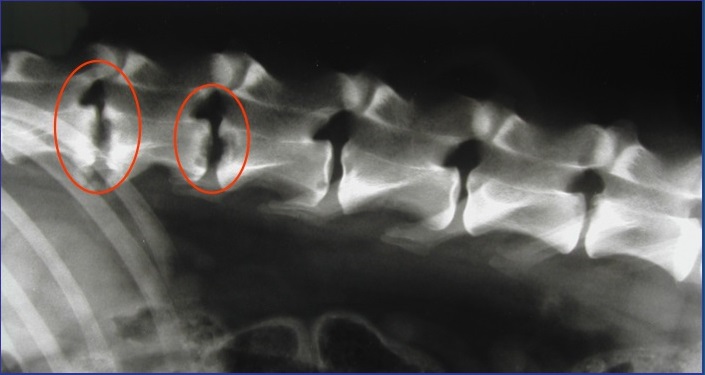
Radiographs (X-rays) of the spine will typically show damage to the vertebrae on either side of the affected discs. In chronic cases, bone changes and deformities of the spine may be seen. Changes may not show up on the radiographs for 3-6 weeks after clinical signs start, so if the first radiographs are normal but the clinical signs are progressing, your veterinarian will likely repeat the radiographs.
If a typical lesion is detected, radiographs of the entire spine are recommended because some pets have multiple lesions. Infection causes disc degeneration and destroys the ends of the adjacent vertebrae. These degenerative changes may weaken the vertebral column and make it susceptible to pathologic fractures, which stem from infection rather than trauma. The body may try to bridge the damaged area with bone, which can encroach on the spinal cord and nerve roots, causing more problems.
Bone scintigraphy, computed tomography (CT), and magnetic resonance imaging (MRI) are more sensitive than plain radiography, particularly for early lesions. Myelography and/or MRI/CT are helpful for pets that have neurological problems, and these imaging methods are considered important if spinal surgery is going to be done.
Culturing the urine, blood, spinal fluid, or other infected tissues may help identify the organism(s) that caused the infection. However, culture of the infected disc space will yield the most accurate results. Fluoroscopic-guided fine needle aspiration may be necessary to get the best sample. If spinal surgery is necessary, samples of the infected areas should be obtained and cultured.
Brucellosis serology (checking the blood for current and previous infections) should be performed. Brucellosis is a possible cause of discospondylitis, and can be transmitted to people.
CSF analysis is called for in animals with neurologic signs. In addition to culturing the CSF, routine cytology, cell count, and protein determination are done.
Causes:
-
Bacteria such as Staphylococcus, Streptococcus, Escherichia coli, and Brucella spp. are commonly isolated organisms. Pseudomonas, Proteus, Pasteurella, Corynebacterium, and Actinomyces spp. are sometimes found. Reproductive problems may occur with Brucella infections. There are reports of pets infected with Bordetella spp., Erysipelothrix rhusiopathiae, and Salmonella spp.
-
Fungal organisms that can cause discospondylitis include Aspergillus, Blastomyces, Histoplasma, Coccidioides spp., and occasionally Paceilomyces. In Europe, infection with Rasamsonia argillacea has been reported. A single case of infection with Westerdykella spp. has also been reported in a German shepherd dog. Fungal infections can be more difficult to diagnose than bacterial infections, so your veterinarian will also look for enlarged lymph nodes, lung or eye lesions, and fungal organisms in the urine.
Treatment/Management/Prevention
Treatment involves a long course of antibiotics that are specific for the infective organism. Ideally, the antibiotic selection will be based on culture and sensitivity results from the infected disc. If disc culture is not possible, then antibiotic selection will be based upon the culture results of urine, blood, or other infected areas.
Antibiotic treatment may be needed for many months to sometimes greater than a year. Recurrence of the disease or persistence of signs can be a problem if antibiotic therapy is stopped too soon, if the antibiotic being used is ineffective, or if corticosteroids or other immunosuppressive drugs are used.
Antifungal drugs, particularly itraconazole, may be effective for treating some cases of fungal discospondylitis.
Surgical exploration of the region may be recommended to obtain a better culture. Decompressive surgery and/or stabilization may be considered if evidence of spinal cord compression is found on myelography or MRI, or if severe, progressive neurologic problems occur.
If antibiotics are effective, pain medications may be needed for only a few days.
Monitoring and Prognosis
After your pet has had at least 6-12 weeks of therapy, your veterinarian may take more radiographs to see if the lesions have improved. Improvement of clinical signs often occurs before improvement can be seen on the radiographs. C-reactive protein is a blood marker of inflammation which can be used to monitor disease as well. Prognosis for recovery is guarded and depends, to some degree, on the cause of the discospondylitis.
